You don’t have cysts, so it may not be PCOS. For years, women have been dealing with missed periods, stubborn weight, acne in adulthood, hair thinning at the crown, and constant exhaustion. Doctors look at an ultrasound, see no cysts, and essentially close the file. They are dismissed and told to come back if things get worse. The problem, it appears, was with the name of the condition.
On 12 May 2026, a global consortium of more than 50 medical and patient organisations officially retired the term Polycystic Ovary Syndrome and replaced it with a new one: Polyendocrine Metabolic Ovarian Syndrome, or PMOS. The announcement was published in The Lancet and presented at the European Congress of Endocrinology in Prague. It followed more than a decade of consultations involving roughly 22,000 doctors, researchers, patients, and advocates across the world. The conclusion they reached was not complicated: the old name was misleading, and that had consequences.
See Also: 4 in 10 Women Have Tried to Change Their Bodies Because of Social Media

So What Was Wrong With the Name PCOS And Why Did It Need To Change?
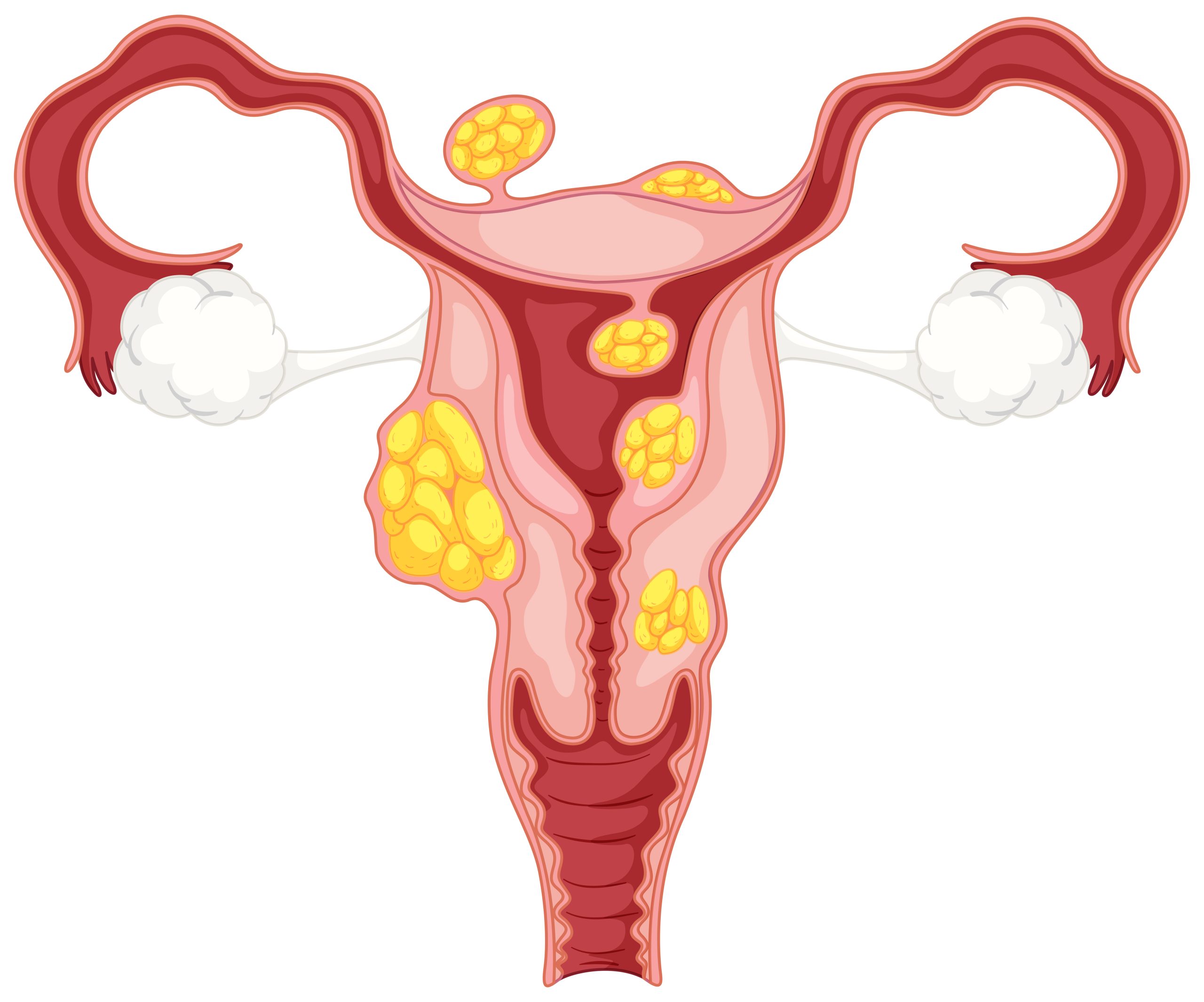
The name Polycystic Ovary Syndrome pointed directly at the ovaries and implied that cysts were the defining feature of the condition. Neither of those things is accurate. The condition is not primarily about the ovaries. And you do not need cysts to have it.
What PCOS, now PMOS actually is, is a hormonal and metabolic disorder. Multiple hormone systems are involved, not just the reproductive ones. The ovaries are affected, yes, but they are one piece of a much larger picture that includes insulin resistance, inflammation, cardiovascular risk, and mental health. A name that put cysts at the centre of all of that was always going to mislead, and it did for decades.
The new name breaks down more honestly. Polyendocrine means multiple endocrine or hormone systems are involved. Metabolic captures the condition’s effects on the body’s processing of insulin, weight regulation, and diabetes risk. Ovarian acknowledges that it does affect the ovaries, ovulation, and periods. Syndrome signals that this is not one disease with one clear presentation, it is a cluster of overlapping symptoms and health risks that can look different in different bodies.
What Is Actually Happening in the Body
At the centre of PMOS is a hormonal miscommunication. In many women with the condition, the body produces too much insulin. That excess insulin then signals the ovaries to produce too much testosterone. That testosterone is what throws reproductive hormones out of balance, disrupting ovulation, causing irregular or absent periods, and triggering the androgen-related symptoms like acne, facial hair growth, and hair thinning on the scalp.
The full symptom picture is broader than most people realise. Irregular or missed periods are the most commonly recognised sign, but the condition also presents as elevated androgen levels, weight gain that concentrates around the abdomen, difficulty getting pregnant, dark patches of skin around the neck or underarms, and persistent hormonal acne. More recently, the clinical understanding of PMOS has been expanded to formally include sleep apnoea, depression, anxiety, and body dysmorphia as part of the condition’s reach.
According to the Cleveland Clinic, diagnosis is made when a patient presents at least two of three markers: irregular or absent ovulation, signs of elevated androgens (either through blood tests or physical symptoms), or polycystic ovarian morphology on an ultrasound. That last one, the cysts, is just one of three criteria. It is not required. It has never been required. But because the name said otherwise, women were not diagnosed properly.
See Also: An Expert View On How The Heat Affects Your Hormones
The Nigerian Reality
Globally, PMOS affects 1 in 8 women of reproductive age. In Nigeria, the numbers are comparable. A community-based study conducted across Mushin and Surulere in Lagos found that at least 8.6% of unselected Nigerian women of reproductive age had the condition. Other studies using the Rotterdam diagnostic criteria, the standard clinical tool for diagnosis, found prevalence rates of 12.2% and 18.1% among different Nigerian populations.
Those are not small numbers. That is a significant portion of Nigerian women walking around with a condition that may be shaping their periods, their skin, their weight, their fertility, their mental health, and in many cases, not knowing it.
Part of the problem is structural. There have been very few systematic studies of this condition in sub-Saharan Africa, which has limited the ability to build proper screening and public health approaches for the region. Nigerian doctors are working with the same inadequate name and the same gaps in research that have affected diagnosis everywhere else. Research in Nigerian university populations has found that while women have some awareness of the condition’s symptoms, knowledge about its long-term risks is limited, stigma around healthcare-seeking remains a barrier, and actual screening uptake is low even among women who are willing to go.
There is also the cultural layer. In Nigeria, symptoms like weight gain, irregular periods, and fertility difficulties do not exist in a vacuum. A woman who is struggling to conceive is not simply navigating a medical issue, she is often navigating family pressure, questions she did not ask for, and a silence around what her body is doing that has been treated as shameful rather than medical. Research across multiple countries has found that more than half of women with PMOS reported feeling less feminine because of symptoms related to weight and fertility. The Nigerian woman with this condition has rarely had her experience named, let alone treated with the seriousness it deserves.

Why the PCOS Name Change Matters
An estimated 70% of people with this condition do not know they have it. That figure alone tells you that the old name was not doing its job. Studies have found that a third of women with PMOS visited multiple doctors before receiving a diagnosis. 88% of patients reported being dissatisfied with the care they received. Women described being dismissed, undertreated, or given advice focused entirely on weight loss or fertility management while the underlying condition went unaddressed.
The name was feeding all of that. When a doctor anchors on “polycystic,” they scan an ultrasound for cysts. When they do not find them, many stop looking. When a patient hears “polycystic ovary syndrome,” she assumes the problem is in her ovaries. She does not know to mention the fatigue, the insulin resistance, the anxiety, the dark patches on her skin, because those things do not sound like ovary problems. The name was drawing a box around the condition that left most of its reality outside.
What Changes Now — And What Doesn’t
If you have already been diagnosed with PCOS, your diagnosis does not disappear. Your treatment plan does not change overnight. The rename is being rolled out over three years, with updates to clinical guidelines across 195 countries as the process continues. What changes is the framework, the way this condition is understood, communicated, researched, and taught to the next generation of doctors.
For women who have suspected something was wrong but could not get a clear answer, the shift matters more immediately. A diagnostic framework that is no longer built around cysts should, in theory, make it easier to be assessed properly. The question is no longer whether you have the cysts the name implied you must have. The question is whether your hormonal and metabolic picture fits. That is a more honest question, and it opens the door for more women to finally get answers.
If you suspect you may have PMOS, the path forward is a visit to a gynaecologist or endocrinologist who can assess your hormone levels, your menstrual history, and your metabolic markers, including blood glucose and insulin levels. Do not go in asking about cysts. Go in describing your full symptom picture, and ask to be assessed against the Rotterdam criteria.
The medical system took a long time to admit the name was wrong. The least it can do now is diagnose you correctly.